Health
Stroke cases in Malaga province have risen by 32% since the outbreak of Covid-19 pandemic
Health experts believe that this figure has several explanations, ranging from more complete and faster diagnoses to some effects of the virus itself

February 2025 marks five years since the first cases of Covid-19 were registered in Spain. Five years in which medicine has been able to defeat a pandemic in record time, although the real scope of the consequences will probably not be known for some time. However, at the moment it is possible to analyse some figures and data compiled from different sources. One of the figures marks the exponential increase in cardiovascular cases, which, in the case of strokes just in Malaga province, has grown by more than 30% in just four years
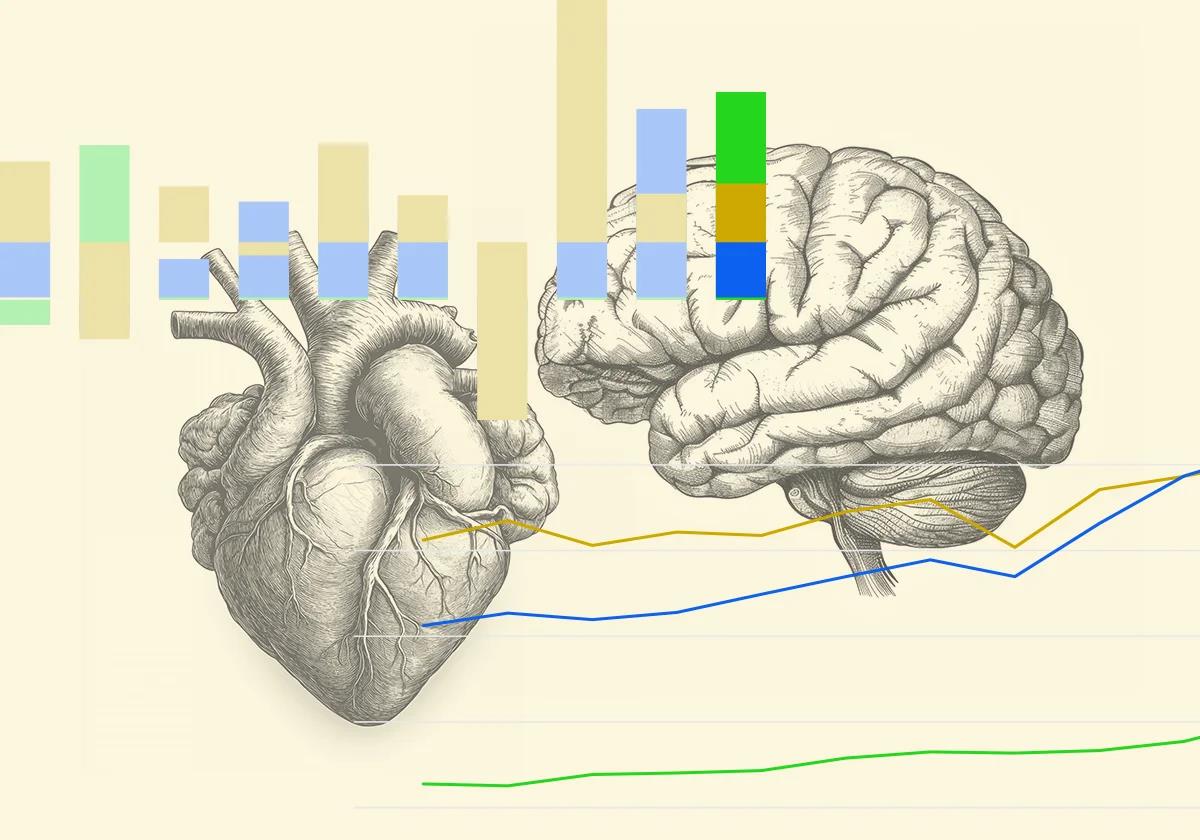
According to official data provided by the Junta de Andalucía's health department, the number of ischaemic strokes registered in the province shot up by 32% (from 1,945 to 2,585 diagnoses) between 2019 and 2023. The full data from 2024 has not yet been revealed. It is true that the general trend over the last decade is upward, but there is a significant acceleration from 2021 onwards, in the second part of the pandemic.
The largest year-on-year increase happened between 2020 and 2021 (by 16.8%), followed by continued growth in 2022 (12.8%). However, growth in 2023 was only 6.2%, compared to the steady growth that had been taking place before the coronavirus began to wreak havoc.
Although it seems that the most affected age group is that between 20 and 39, with an increase of 60%, in quantities this represents an increase from 25 cases in 2019 to 40 in 2023. The most affected group in absolute terms is the over-65s, who go from 1,351 diagnoses to 1,854, i.e. 37.2% increase.
Although ischaemic strokes have grown the most, the increase in haemorrhagic strokes is to not be neglected, marking a growth of 22.5% from 2019 to 2023. In this case, the highest year-on-year increase was in 2023 (by 14.1%). There are no significant changes in the under-19s or in the 20-39 age group, but there is a 32.4% increase in adults aged 40-64.
According to the data accessed by SUR, the cases of acute myocardial infarctions have grown by 10.1%. There have been some fluctuations in this area, with a decrease of 12.1% in 2020, followed by a recovery of 16.7% in 2021. Undoubtedly, the lack of diagnoses during the pandemic explains this drop in the worst year of Covid. The under-40 age group is the only one to have reduced its incidence (-19.4%). Although still rising, the trend here is more stable compared to strokes.
Several factors
What are the reasons behind this statistical anomaly? Experts agree that there is no single reason, although their opinions concerning the relevance of one factor or another vary. Accordingly, Dr Jesús Romero Imbroda, head of neurology at Hospital Quirónsalud Málaga, has stated that it is a "multifactorial" issue. Romero specifically referred to increasing age, i.e. the ageing of the population, as one of the main culprits. This could explain part of the data, but not all of it, as the increase in two years has been exponential.
"I sincerely believe that we are diagnosing strokes earlier, more and better," said Dr. Romero, adding that part of the success is thanks to a wider societal awareness of the importance of early detection of symptoms. "We have put the focus, both in public and private healthcare, on improved care, with increasingly specific protocols and professionals," he stated. Analysing the data, Dr. Romero added: "This increase is probably also related to a possible change in data collection in large hospitals after the pandemic. I would define it as a 'virtue of the system'."

Diferencias entre un
ictus isquémico y un
ictus hemorrágico
El isquémico se produce
por una obstrucción
de la arteria (trombo)
Placa de ateroma
Flujo sanguíneo
El trombo interrumpe
el flujo
La obstrucción también se puede producir por un coágulo desprendido de
un trombo en
el corazón
Arteria
carótida
Arteria
vertebral
El hemorrágico se produce por la
hemorragia dentro del cerebro
por una rotura de la arteria
Rotura de la arteria
Flujo
sanguíneo
Rotura de un
aneurisma
Tanto si es un ictus isquémico como si
es hemorrágico, los síndromes varían
según el lugar del cerebro donde
se encuentre la arteria afectada
Arteria
cerebral
anterior
Arteria
cerebral
posterior
Disminución
de la actividad
psicomotora y
de la fuerza y
sensibilidad en
la mitad del cuerpo
(sobre todo,
en la pierna)
Pérdida
de visión
en la mitad
del campo
visual y
dificultad
en el
lenguaje
Arteria
cerebral
media
Pérdida de
visión en la
mitad del
campo visual y dificultad en el lenguaje; disminución de la fuerza y la sensibilidad en la mitad del cuerpo
Fuente:
Clínica Universidad de Navarra
Diferencias entre un ictus isquémico
y uno hemorrágico
El isquémico se produce
por una obstrucción
de la arteria (trombo)
Placa de ateroma
Flujo sanguíneo
El trombo interrumpe
el flujo
La obstrucción también se puede producir por un coágulo desprendido de
un trombo en
el corazón
Arteria
carótida
Arteria
vertebral
El hemorrágico se produce por la
hemorragia dentro del cerebro
por una rotura de la arteria
Rotura de la arteria
Flujo
sanguíneo
Rotura de un
aneurisma
Tanto si es un ictus isquémico como si
es hemorrágico, los síndromes varían
según el lugar del cerebro donde
se encuentre la arteria afectada
Arteria
cerebral
anterior
Arteria
cerebral
posterior
Disminución
de la actividad
psicomotora y
de la fuerza y
sensibilidad en
la mitad del cuerpo
(sobre todo,
en la pierna)
Pérdida
de visión
en la mitad
del campo
visual y
dificultad
en el
lenguaje
Arteria
cerebral
media
Pérdida de
visión en la
mitad del
campo visual y dificultad en el lenguaje; disminución de la fuerza y la sensibilidad en la mitad del cuerpo
Fuente: Clínica Universidad de Navarra
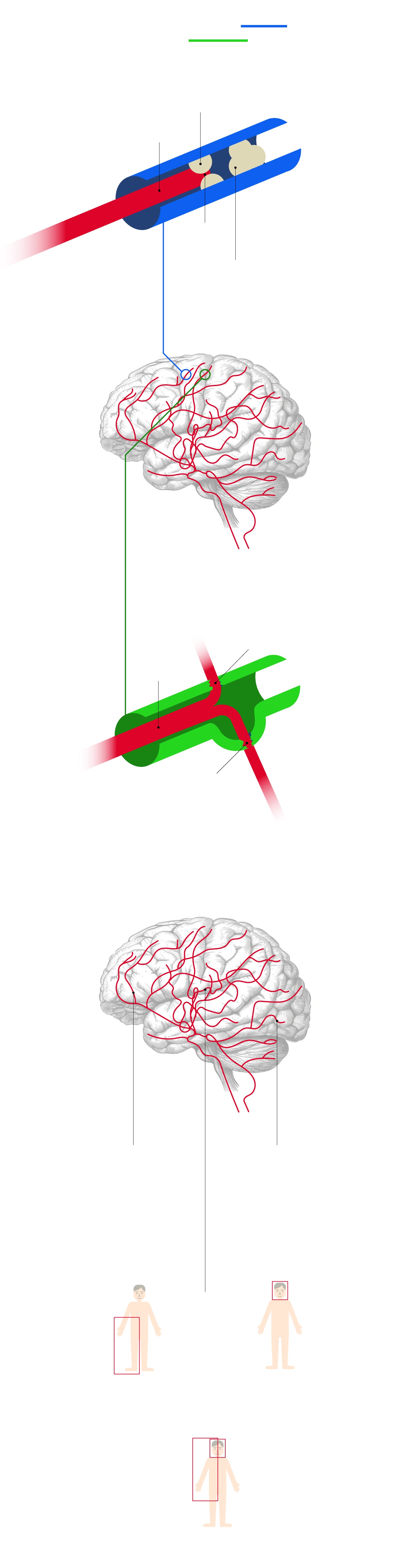
Diferencias entre un ictus isquémico y un ictus hemorrágico
El isquémico se produce
por una obstrucción
de la arteria (trombo)
El hemorrágico se produce
por la hemorragia dentro del cerebro
por una rotura de la arteria
Placa de ateroma
Rotura de la arteria
Flujo sanguíneo
Flujo sanguíneo
El trombo interrumpe
el flujo
Rotura de un
aneurisma
La obstrucción también se puede producir por un coágulo desprendido de
un trombo en
el corazón
Tanto si es un ictus isquémico como si
es hemorrágico,
los síndromes varían
según el lugar del cerebro donde se encuentre la
arteria afectada
Arteria
carótida
Arteria
vertebral
Arteria
cerebral
media
Arteria
cerebral
anterior
Arteria
cerebral
posterior
Pérdida de visión en la mitad del campo visual y dificultad en el lenguaje; disminución de la fuerza y la sensibilidad en la mitad del cuerpo
Disminución
de la actividad psicomotora y de la fuerza y sensibilidad en la mitad del cuerpo (sobre todo, en la pierna)
Pérdida de
visión en
la mitad del campo visual
y dificultad
en el lenguaje
Fuente: Clínica Universidad de Navarra
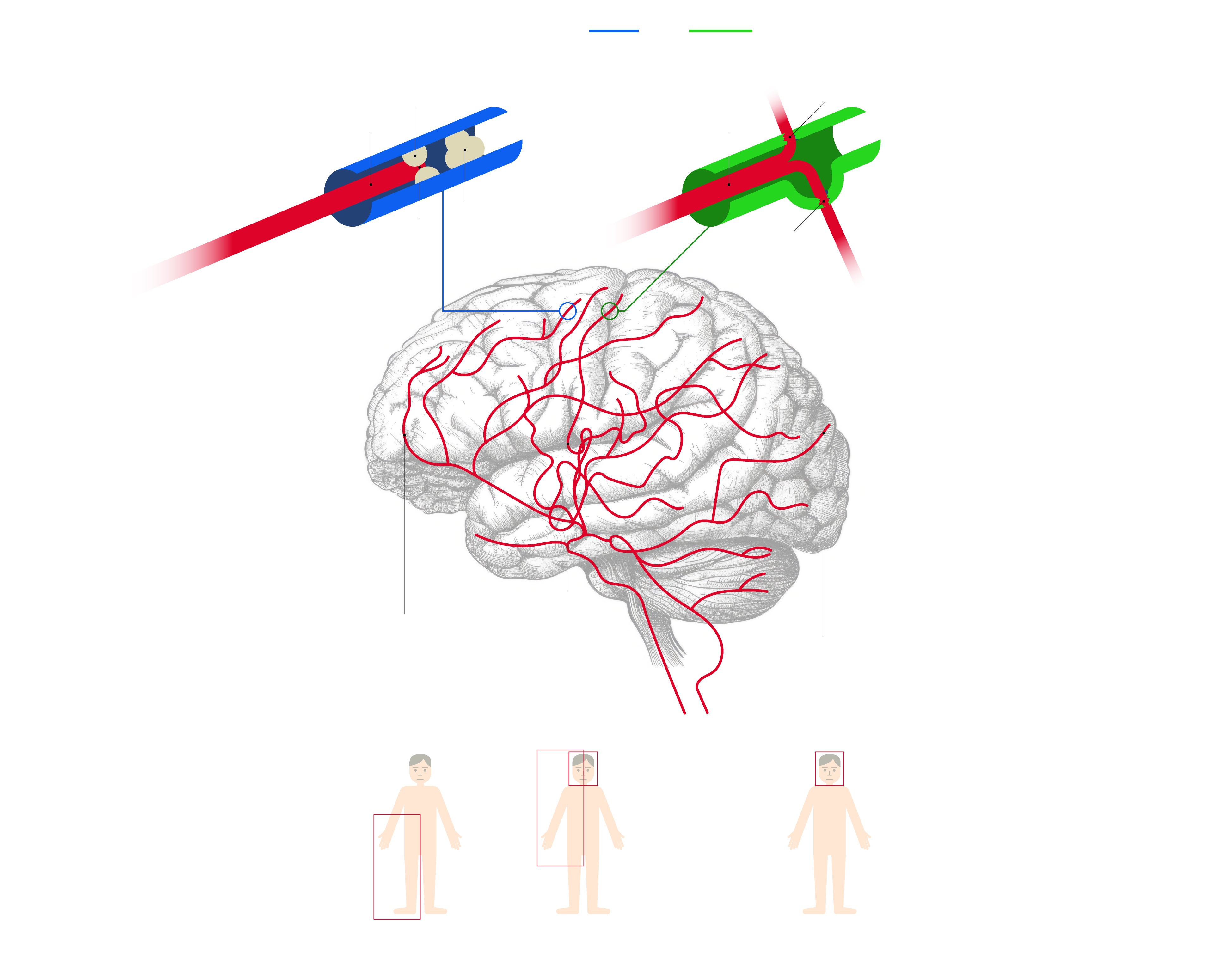
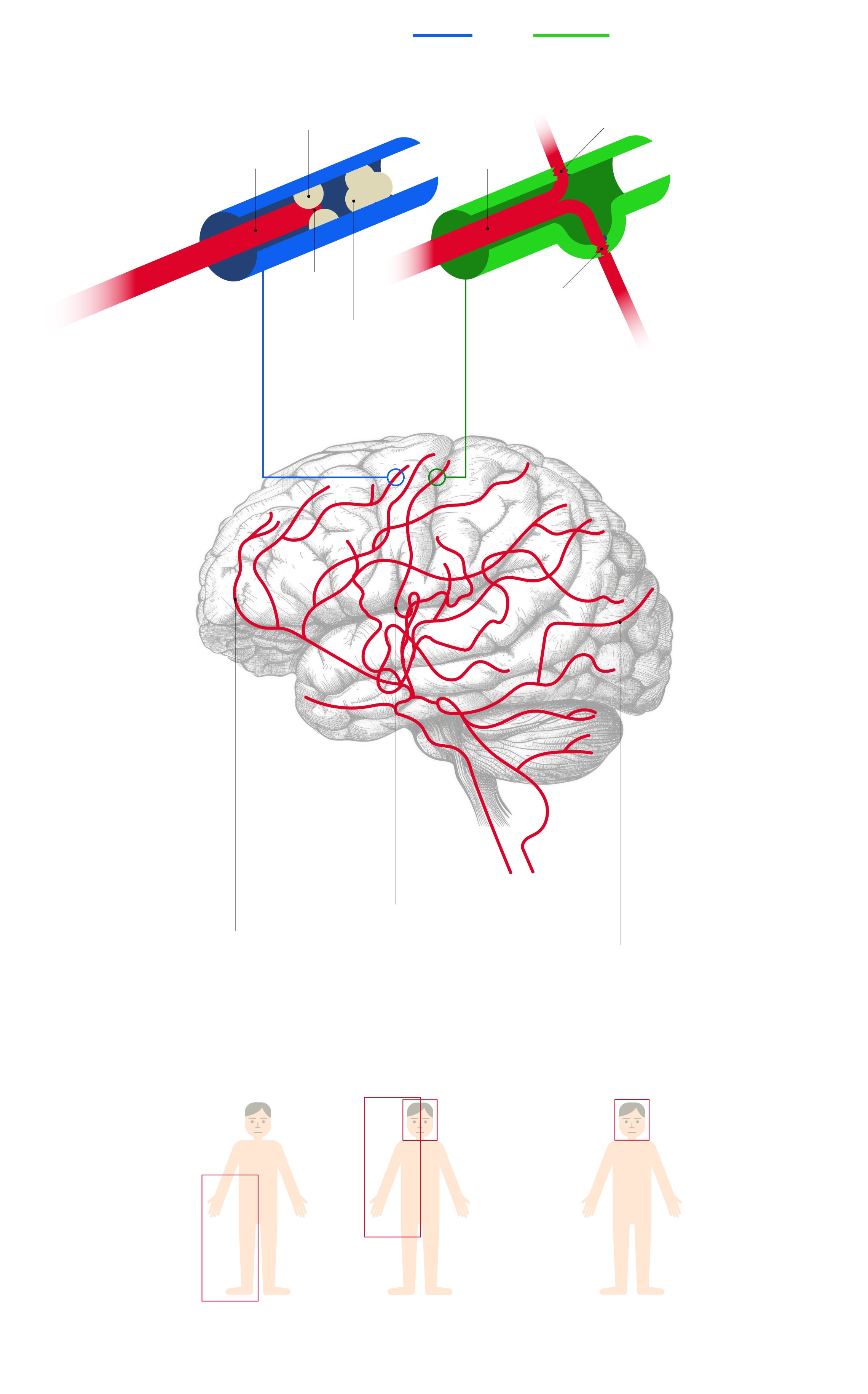
Diferencias entre un ictus isquémico y un ictus hemorrágico
El isquémico se produce por una obstrucción de la arteria (trombo)
El hemorrágico se produce por la hemorragia dentro del cerebro por una rotura de la arteria
Rotura de la arteria
Placa de ateroma
Flujo sanguíneo
Flujo sanguíneo
La obstrucción también
se puede producir por un coágulo desprendido de
un trombo en el corazón
El trombo interrumpe
el flujo
Rotura de un
aneurisma
Tanto si es un ictus isquémico como si
es hemorrágico,
los síndromes varían
según el lugar del cerebro donde se encuentre la
arteria afectada
Arteria
cerebral
media
Arteria
cerebral
anterior
Pérdida de visión en la mitad del campo visual y dificultad en el lenguaje; disminución de la fuerza y la sensibilidad en la mitad del cuerpo
Arteria
cerebral
posterior
Disminución
de la actividad psicomotora y de la fuerza y sensibilidad en la mitad del cuerpo (sobre todo, en la pierna)
Pérdida de visión en la mitad del campo visual
y dificultad en
el lenguaje
Arteria
carótida
Arteria
vertebral
Fuente: Clínica Universidad de Navarra
What about the pandemic? Although he referred to the virus and everything related to it as a contributing factor, Dr. Romero didn't consider it one that has been "particularly decisive". He did admit that there have been cases of under-diagnosis (especially at the worst time in 2020) and that there has also been a certain relationship with the increase in mental health problems. "Ultimately, I think that now people are consulting more and faster, like when they have a tingling sensation, for example," he said. Addressing widespread concerns regarding the risk of vaccination, the medical expert stated: "The covid vaccine is not the reason for more strokes. The only one with a certain risk was the Astra Zeneca vaccine, for which it has been withdrawn."
Strokes and Covid
Dr José Antonio Trujillo, vice-president of the Malaga College of Physicians and an expert in analysing the consequences of the pandemic, referred to research led by the Cleveland Clinic and the University of Southern California, subsequently published in the journal Arteriosclerosis, Thrombosis and Vascular Biology (ATVB). The study reveals how long the possible increased risk of stroke from Covid lasts and whether it reverses after overcoming the infection. After analysing the data, the researchers found that, during the three-year follow-up period, the risk of heart attack, stroke and death was more than two times higher among adults with Covid-19, and almost four times higher among adults hospitalised with the virus, compared to the group with no history of infection.
In addition, it was observed that hospitalisation was associated with an equivalent risk to coronary artery disease. Specifically, individuals hospitalised with the virus who had no prior history of cardiovascular disease or type 2 diabetes were found to have a 21% higher risk of myocardial infarction, stroke, and death, compared to those with such a history but without a coronavirus infection. Furthermore, according to the study, the increased risk of thrombotic events (myocardial infarction or stroke) among hospitalised Covid-19 cases was found to be due to a genetic interaction with ABO blood group antigens. In fact, according to the research, patients with blood groups A, B or AB hospitalised due to the virus had an approximately 65% higher risk of adverse episodes than subjects with blood group O.
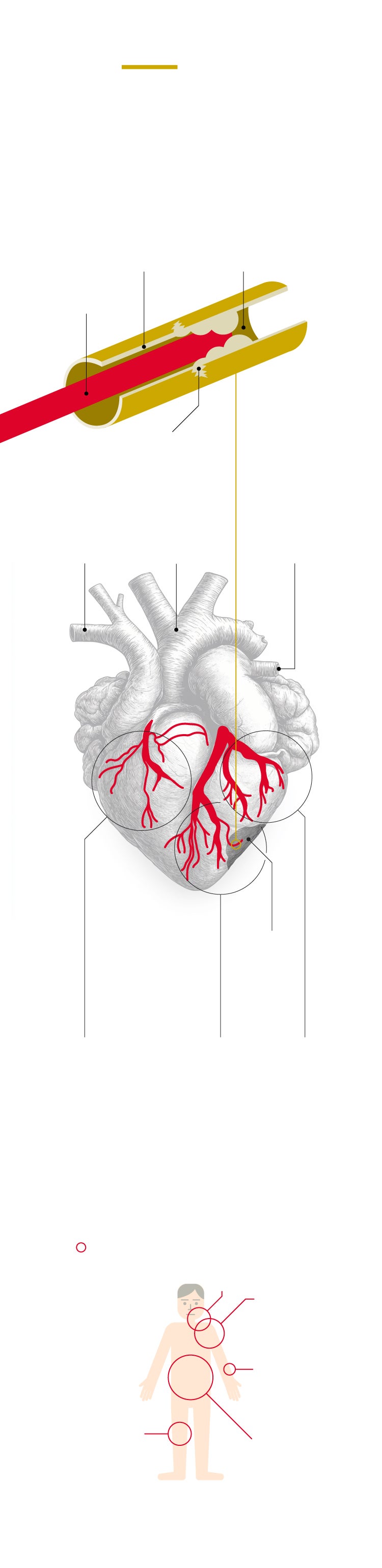
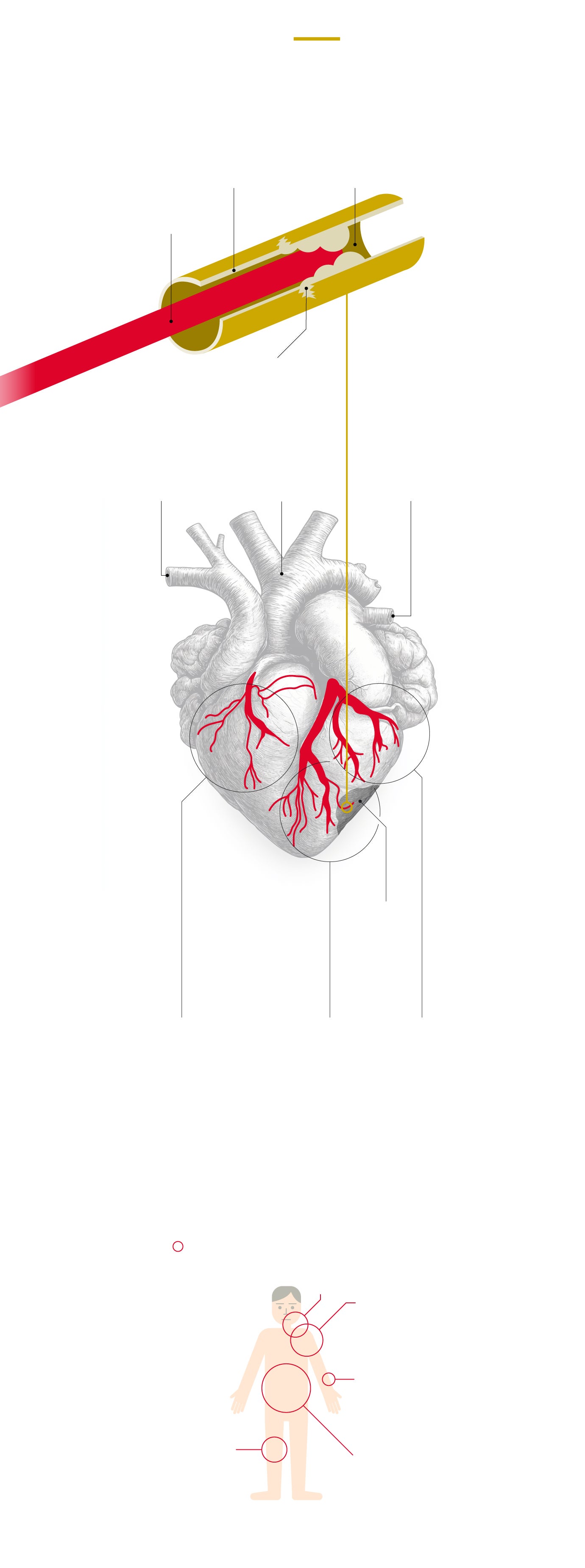
Cómo se produce
un infarto de miocardio
Normalmente se produce
por un trombo (obstrucción) de
una de las arterias coronarias
que conducen el flujo
sanguíneo al músculo
Se reduce
el flujo sanguíneo
o, incluso,
se detiene
Placa de
aterosclerosis
Flujo
sanguíneo
La rotura de
esta placa
provoca
un trombo
Vena
cava
Arteria
pulmonar
Aorta
Miocardio
Músculo
del corazón
La gravedad del infarto depende del lugar donde se localice la arteria coronaria afectada
Necrosis
Arteria coronaria derecha
Arteria descendente anterior
Arteria circunfleja
Síntomas y gravedad intermedios
Síntomas atípicos y gravedad leve
Síntomas evidentes y gravedad alta
Sintomatología
El dolor es el principal síntoma
Porcentaje
de infartos
con dolor
en cada
zona
Mandíbula
y cuello
20%
Brazo izquierdo
y cuello
33%
Brazo izquierdo
5%
Otras zonas o sin dolor
Centro
del pecho
20%
75%
Fuente:
Clínica Universidad de Navarra
Cómo se produce un infarto de miocardio
Normalmente se produce por un trombo (obstrucción) de una de las arterias coronarias
que conducen el flujo sanguíneo al músculo
Se reduce el flujo
sanguíneo o, incluso,
se detiene
Placa de
aterosclerosis
Flujo
sanguíneo
La rotura de
esta placa
provoca
un trombo
Vena
cava
Arteria
pulmonar
Aorta
Miocardio
Músculo
del corazón
La gravedad del infarto depende del lugar donde se localice la arteria coronaria afectada
Necrosis
Arteria coronaria derecha
Arteria descendente anterior
Arteria circunfleja
Síntomas y gravedad intermedios
Síntomas atípicos y gravedad leve
Síntomas evidentes y gravedad alta
Sintomatología
El dolor es el principal síntoma
Porcentaje
de infartos
con dolor
en cada
zona
Mandíbula
y cuello
20%
Brazo izquierdo
y cuello
33%
Brazo izquierdo
5%
Otras zonas o sin dolor
Centro
del pecho
20%
75%
Fuente: Clínica Universidad de Navarra
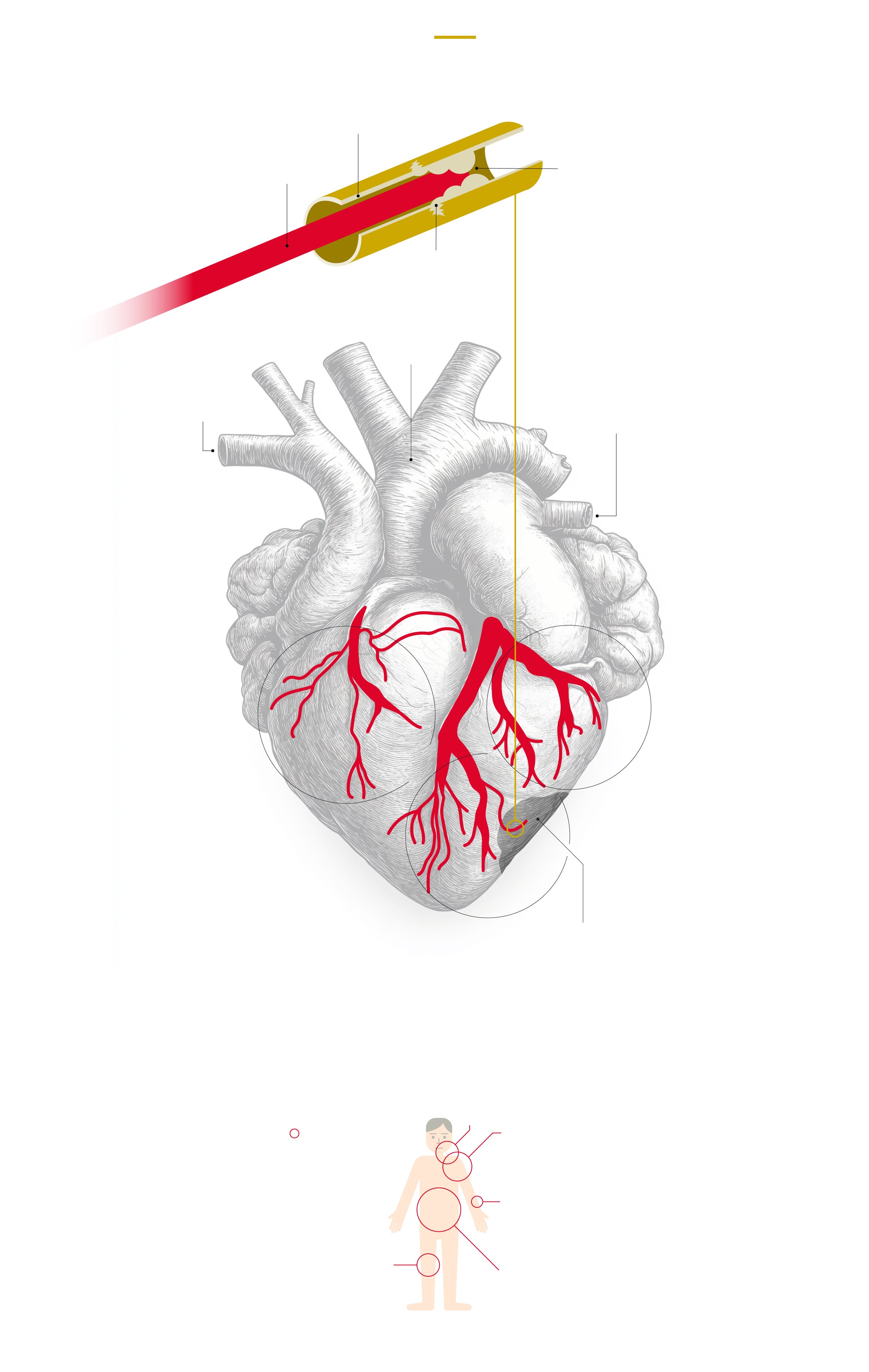
Cómo se produce un infarto de miocardio
Normalmente se produce por un trombo
(obstrucción) de una de las arterias coronarias
que conducen el flujo sanguíneo al músculo
Placa de aterosclerosis
Se reduce el flujo
sanguíneo o, incluso,
se detiene
Flujo sanguíneo
La rotura de
esta placa
provoca
un trombo
Aorta
Vena
cava
Arteria pulmonar
Miocardio
Músculo
del corazón
Arteria coronaria derecha
Arteria circunfleja
Síntomas atípicos y gravedad leve
Síntomas y gravedad intermedios
La gravedad del infarto depende del lugar donde se localice la arteria coronaria afectada
Arteria descendente anterior
La falta de riego sanguíneo de manera prolongada en la zona puede provocar cambios irreversibles e, incluso, necrosis (muerte del tejido)
Síntomas evidentes y gravedad alta
Sintomatología
Mandíbula
y cuello
El dolor es el principal síntoma
20%
Brazo izquierdo
y cuello
Porcentaje
de infartos
con dolor
en cada zona
33%
Brazo izquierdo
5%
Otras zonas o sin dolor
Centro
del pecho
20%
75%
Fuente: Clínica Universidad de Navarra
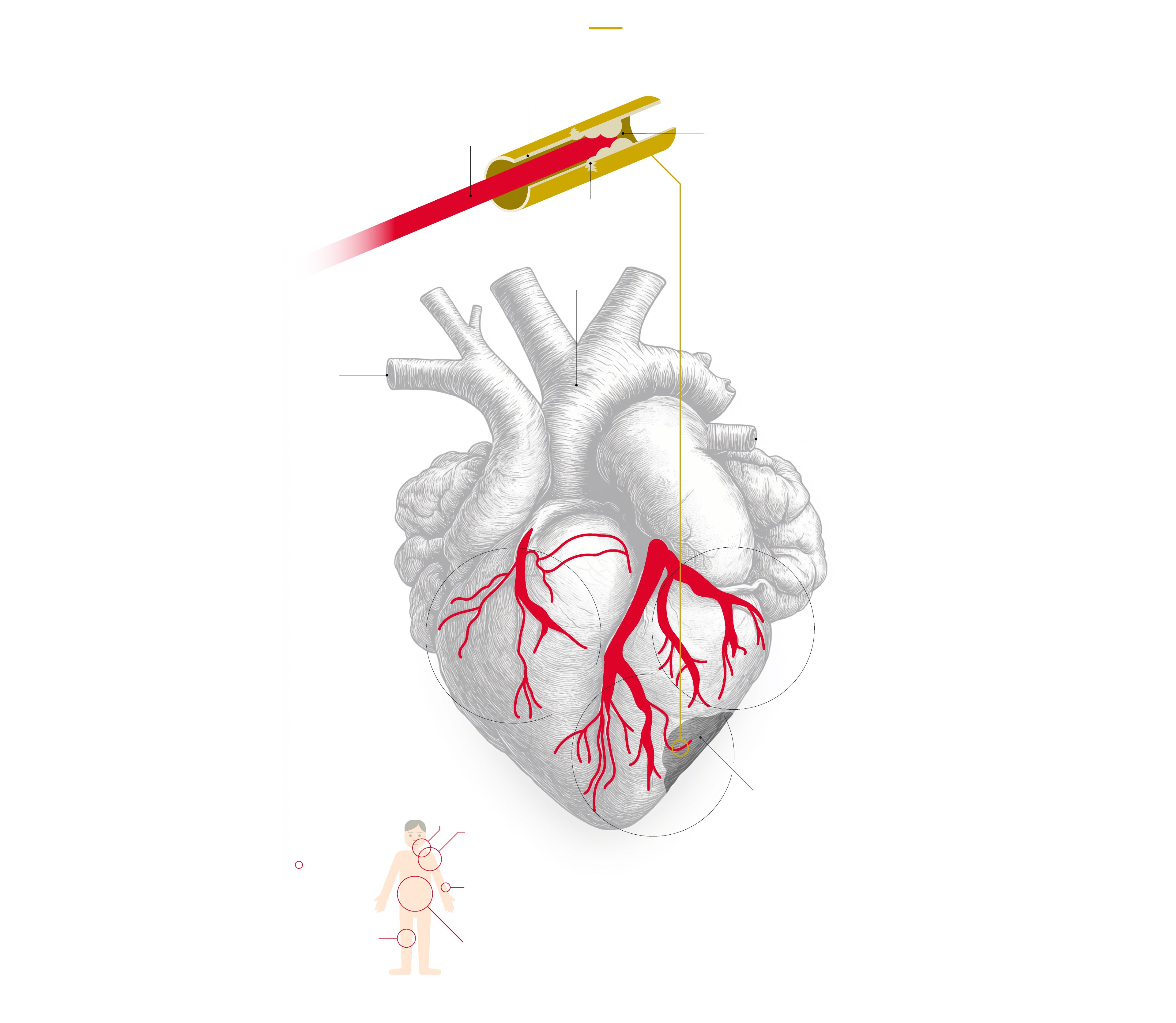
Cómo se produce un infarto de miocardio
Normalmente se produce por un trombo
(obstrucción) de una de las arterias coronarias
que conducen el flujo sanguíneo al músculo
Placa de aterosclerosis
Se reduce el flujo
sanguíneo o, incluso,
se detiene
Flujo sanguíneo
La rotura de
esta placa
provoca
un trombo
Aorta
Vena cava
Arteria pulmonar
La gravedad del infarto depende del lugar donde se localice la arteria coronaria afectada
Miocardio
Arteria coronaria derecha
Músculo
del corazón
Arteria circunfleja
Síntomas atípicos y gravedad leve
Síntomas y gravedad intermedios
La falta de riego sanguíneo de manera prolongada en la zona puede provocar cambios irreversibles e, incluso, necrosis (muerte del tejido)
Mandíbula
y cuello
20%
Sintomatología
Brazo izquierdo
y cuello
El dolor es el principal síntoma
Arteria descendente anterior
Porcentaje
de infartos
con dolor
en cada zona
33%
Brazo izquierdo
Síntomas evidentes y gravedad alta
5%
Otras zonas o sin dolor
Centro
del pecho
20%
75%
Fuente: Clínica Universidad de Navarra
Better diagnostics
Just under a decade ago, Malaga's Hospital Regional introduced thrombectomy - a highly effective treatment for stroke - which meant that the majority of cases in the province ended up being referred to this hospital. Neurologist Rafael Bustamante, head of stroke, stated that the increase in diagnoses has grown exponentially, specifically in this health centre. "It is difficult to discern which increase is due to a change in the protocol, and which is due to the increase in the number of cases," he said.
According to Bustamante, strokes have been increasing in the last decade due to a greater prevalence of negative lifestyles, such as hypertension, obesity or stress. In his opinion, the important thing is to study the aetiology, i.e. the cause. "If you know how it happened, you know how to prevent it," he reminded. The aforementioned study includes cryptogenic strokes, which are those of 'unknown' origin. "There we did not find any increase that has to do with strange issues, such as the coronavirus vaccine or the virus itself," said Dr Bustamante, admitting that, during the first waves of the pandemic, we saw strokes in the acute phase, after which the famous thrombotic complication of the Astrazeneca vaccine appeared. "But rather than an increase in cases, what we saw during the pandemic were more severe cases. Once that was over, we did not notice an increase in patients with strokes of unknown origin. In fact, the percentage of strokes with no known cause is decreasing," he said.
Dr Bustamante stated that what has changed in recent times is the fact that patients are being studied more. "That is why we are detecting more problems than ever, such as a recurrent cardiac septal defect that causes strokes, or atrial fibrillations and thrombophilia states," he noted.
So why is there this statistical anomaly in the increase of cases? A single explanation would be "too simple", said the neurologist. "The fear of the virus and the vaccines started because of the thrombotic phenomena they could cause. This presented a very catastrophic picture that did not go unnoticed, but we have not seen such a large increase to explain the statistics. It is possible that factors such as obesity or hypertension have increased as a result of the pandemic. We should not forget that the more obesity, the more hypertension and the more strokes," stated Dr Bustamante.
He also believes that the focus should be placed on drug use, although in a relative way because the percentage is small. "I put it down more to lifestyle changes and the increase in risk factors," he said. "We diagnose much better than before, more extensively and in more age groups. Not so long ago, stroke was not diagnosed in people under 30 years of age. Now there is more awareness that they can occur at any age."